What is a systematic review? How to conduct and write a systematic review
Key takeaways
- A systematic review is a thorough and detailed review of existing literature on a particular topic, designed to address a specific question.
- Systematic reviews are especially important in evidence-based medicine.
- A good systematic review begins with a protocol that defines the study design, objectives, and expected outcomes; follows the PRISMA guidelines, and should be registered in a recognized protocol registry.
This article covers the basics of how to approach a systematic review and how such a review is typically structured.
Jump to Contents
- What is a systematic review?
- What is the difference between a systematic review and a literature review?
- What are the types of systematic reviews?
- How to write a protocol for a systematic review?
- What is the best approach to conducting a systematic review?
- How is a systematic review article structured?
- Sample structure of a systematic review
- How do I manage references for a systematic review?
What is a systematic review?
A systematic review is a highly rigorous review of existing literature that addresses a clearly formulated question. The review systematically searches, identifies, selects, appraises, and synthesizes research evidence relevant to the question using methodology that is explicit, reproducible, and leads to minimum bias.
What is the difference between a systematic review and a literature review?
| Aspect | Systematic review | Literature review |
| Purpose | Answer a specific, pre-defined research question by synthesising all available evidence. | Provide a broad overview or background on a topic, often to contextualise a study. |
| Search strategy | Exhaustive, documented search across multiple databases with predefined inclusion/exclusion criteria. | Selective and flexible; researcher chooses sources based on relevance and familiarity. |
| Reproducibility | Highly reproducible: another researcher following the same protocol should reach the same results. | Not typically reproducible; reflects the author’s interpretation and selection of sources. |
| Team & time | Usually requires multiple reviewers and significant time due to screening and quality appraisal. | Can be done by a single researcher in a shorter timeframe; common in theses and papers. |
| Output & bias | Evidence synthesis with bias minimised; may include meta-analysis for quantitative pooling. | Narrative summary; more susceptible to selection bias and the author’s perspective. |
What are the types of systematic reviews?
- Prognostic reviews: examine factors that predict the course or outcome of a condition in a defined population.
- Qualitative systematic reviews: synthesize qualitative research to explore experiences, perceptions, or meanings rather than numerical outcomes.
- Mixed-methods reviews: combine quantitative and qualitative evidence to provide a more complete picture of a topic.
- Scoping reviews: map the breadth of evidence on a topic, identify gaps, and clarify concepts; less focused on a single question than a traditional systematic review.
- Rapid reviews: follow systematic review methods but with a streamlined process to produce findings faster, often for policy decisions.
- Umbrella reviews (reviews of reviews): synthesize evidence from multiple existing systematic reviews on the same broad topic.
- Network meta-analyses: a specialized type that compares multiple interventions simultaneously, even when they haven’t been directly compared in trials, using indirect evidence.
- Individual patient data (IPD) reviews: use raw data from individual participants across studies rather than aggregate published results, allowing more precise analysis.
How to write a protocol for a systematic review?
Any good systematic review begins with a protocol. According to the National Institutes of Health (NIH), a protocol serves as a road-map for your review and specifies the objectives, methods, and outcomes of primary interest of the systematic review. The purpose of having a protocol is to promote transparency of methods.
What does the protocol contain?
A protocol defines the search terms, inclusion and exclusion criteria, data that will be analyzed, etc. The protocol needs to be submitted to the journal along with your manuscript.
A protocol ideally includes the following:
- Databases to be searched and additional sources (particularly for grey literature)
- Keywords to be used in the search strategy
- Limits applied to the search.
- Screening process
- Data to be extracted
- Summary of data to be reported
Most journals expect authors of systematic reviews to use the PRISMA statement or similar other guidelines to write their protocol.
What is the PRISMA statement?
The PRISMA Statement is a document that consists of a 27-item checklist and a flow diagram and aims to guide authors on how to develop a systematic review protocol and what to include when writing the review. Anybody writing a systematic literature review should be familiar with the PRISMA statement.
Should I register a systematic review protocol?
Once you have written your protocol, it is advisable to register it. Registering your protocol is a good way to announce that you are working on a review, so that others do not start working on it.
Where can I register a protocol for a systematic review?
The available protocol registries for systematic reviews are:
- Campbell Collaboration: Specific to systematic reviews of social interventions
- Cochrane Collaboration: Specific to systematic reviews of health care interventions
- PROSPERO: An open registry for all systematic reviews
The registries also provide a searchable database of registered reviews. Before starting a systematic review, you should search these databases for any registered reviews on the topic of your choice. This will ensure that you are not duplicating efforts.
What is the best approach to conducting a systematic review?
The essence of a systematic review lies in being systematic. A systematic review involves detailed scrutiny and analysis of a huge mass of literature. To ensure that your work is efficient and effective, you should follow a clear process:
1. Develop a Research Question
A well-formed research question is the cornerstone of any systematic review. The PICO framework is the standard tool for structuring clinical questions:
| Element | Meaning | Example |
| P: Population | Who is being studied? | Adults ≥18 with heart failure with reduced ejection fraction (HFrEF) |
| I: Intervention | What is being done? | SGLT2 inhibitors (e.g., dapagliflozin, empagliflozin) |
| C: Comparison | Compared to what? | Placebo or standard of care |
| O: Outcome | What is measured? | Cardiovascular death, hospitalization for heart failure, LVEF improvement |
Example research question
“In adults with HFrEF, do SGLT2 inhibitors compared to placebo reduce the risk of cardiovascular death or worsening heart failure?”
A strong research question is specific enough to be answerable yet broad enough to capture sufficient evidence. Avoid questions that are too narrow (“Does dapagliflozin 10mg reduce NT-proBNP at 6 months in NYHA Class III patients in Europe?”) or too vague (“Are heart failure drugs effective?”).
2. Define Inclusion and Exclusion Criteria
Criteria must be defined before searching to prevent bias. They flow directly from the PICO components.
Example inclusion criteria:
- Randomized controlled trials (RCTs) or prospective cohort studies
- Adults diagnosed with HFrEF (LVEF ≤40%)
- Intervention: any SGLT2 inhibitor at any approved dose
- Reporting at least one of: cardiovascular mortality, HF hospitalization, LVEF change, quality of life (KCCQ score)
- Minimum follow-up: 3 months
- Published in English, Spanish, or French
Example exclusion criteria:
- Studies in patients with type 1 diabetes only (distinct pathophysiology)
- Case reports, editorials, conference abstracts without full data
- Studies with <50 participants (underpowered for clinical endpoints)
- Duplicate publications of the same trial cohort
Documenting these criteria in a prospectively registered protocol (e.g., on PROSPERO) before the search begins is considered best practice and protects against selective reporting.
3. Locate Studies
A comprehensive, reproducible search strategy minimizes publication bias. Search multiple databases and grey literature sources.
Key databases for reviews:
- MEDLINE/PubMed: primary biomedical literature
- Embase: broader European and pharmaceutical coverage
- Cochrane Central Register of Controlled Trials (CENTRAL): curated trial database
- ClinicalTrials.gov: registered and completed trials (catches unpublished data)
- WHO ICTRP: international trial registry
Example PubMed search string:
(“heart failure”[MeSH] OR “cardiac failure”[tiab])
AND (“SGLT2 inhibitor”[tiab] OR “sodium-glucose cotransporter 2″[tiab]
OR dapagliflozin[tiab] OR empagliflozin[tiab] OR canagliflozin[tiab])
AND (“randomized controlled trial”[pt] OR “clinical trial”[pt])
Additional strategies:
- Hand-search reference lists of included studies and key review articles
- Contact study authors or pharmaceutical companies for unpublished data
- Search conference proceedings (ACC, ESC, AHA) for late-breaking trials
All searches should be date-stamped, and the full search strategy documented for reproducibility. Involve a medical librarian when possible.
4. Select Studies
Study selection typically occurs in two sequential stages to be both thorough and efficient.
Stage 1: Title and abstract screening
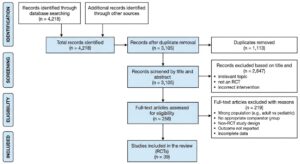
Two reviewers independently screen all retrieved records against the inclusion/exclusion criteria. For a cardiology review on SGLT2 inhibitors, a search may yield 3,000–5,000 records, which are rapidly filtered to ~200–300 potentially relevant studies.
Stage 2: Full-text review
Full-text articles for all potentially eligible studies are retrieved and assessed. Disagreements between reviewers are resolved by consensus or a third arbiter.
Tools used:
- Covidence, Rayyan, or DistillerSR: software platforms that facilitate blinded, parallel screening and track decisions
- PRISMA flow diagram: the standard way to report how many records were identified, screened, excluded, and included
PRISMA Flow (simplified example):
5. Assess Study Quality
Quality (or risk of bias) assessment determines how much confidence to place in each study’s findings. The tool used depends on study design.
For RCTs: Cochrane Risk of Bias Tool 2 (RoB 2) assesses five domains:
| Domain | Example |
| Randomization process | Were patients in DAPA-HF truly randomly allocated? |
| Deviations from intervention | Did control patients receive open-label SGLT2i? |
| Missing outcome data | Was dropout differential between arms? |
| Outcome measurement | Was cardiovascular death adjudicated by a blinded committee? |
| Selective reporting | Were all pre-registered endpoints reported? |
For observational studies: ROBINS-I or the Newcastle-Ottawa Scale are used.
Example assessment
The EMPEROR-Reduced trial (empagliflozin in HFrEF) would typically be rated low risk of bias across most domains: double-blind, placebo-controlled, pre-registered, and with an independent endpoint adjudication committee. In contrast, a single-center retrospective registry study comparing SGLT2i users vs. non-users would rate high risk in the confounding domain.
6. Extract Data
Standardized data extraction forms ensure consistency and completeness. Two reviewers extract independently, then reconcile discrepancies.
What to extract:
Study characteristics:
- Trial name, year, country, funding source, sample size, duration
- Inclusion/exclusion criteria, baseline LVEF, NYHA class, mean age
Intervention details:
- Drug, dose, comparator, background therapy (e.g., beta-blocker use, ACEi/ARB)
Outcomes:
- Primary composite endpoint rates (e.g., CV death + HF hospitalization)
- Effect estimates: hazard ratios (HR), risk ratios (RR), absolute risk differences
- Confidence intervals and p-values
- Subgroup results (diabetic vs. non-diabetic, LVEF range)
Example extracted data row:
| Trial | N | Drug | Follow-up | HR (CV death/HF hosp.) | 95% CI |
| DAPA-HF | 4,744 | Dapagliflozin 10mg | 18.2 mo | 0.74 | 0.65–0.85 |
| EMPEROR-Reduced | 3,730 | Empagliflozin 10mg | 16 mo | 0.75 | 0.65–0.86 |
7. Analyze and Present Results
Narrative synthesis describes patterns across studies qualitatively. Meta-analysis statistically pools effect estimates when studies are sufficiently homogeneous.
Assessing heterogeneity:
- I² statistic: measures the percentage of variability due to true heterogeneity rather than chance
- I² < 25%: low heterogeneity → fixed-effects model appropriate
- I² 25–75%: moderate → investigate sources; random-effects model preferred
- I² > 75%: high → meta-analysis may be inappropriate; consider narrative synthesis only
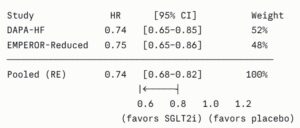
Forest plot (example):
Additional analyses:
- Funnel plots and Egger’s test to assess publication bias
- Subgroup analyses (e.g., with vs. without diabetes, EF 30–40% vs. <30%)
- Sensitivity analyses (e.g., excluding high risk of bias studies)
- Certainty of evidence (GRADE): rates evidence as high, moderate, low, or very low based on risk of bias, inconsistency, indirectness, imprecision, and publication bias
8. Interpret Results
Interpretation goes beyond reporting statistics; it contextualizes findings for clinical and policy decision-making.
Key questions to address:
Clinical significance vs. statistical significance: A pooled HR of 0.74 for CV death/HF hospitalization with SGLT2 inhibitors is both statistically significant and clinically meaningful — translating to a number needed to treat (NNT) of approximately 19 over 18 months to prevent one primary event.
Generalizability: The landmark SGLT2i trials enrolled predominantly male patients (~75%) with well-controlled diabetes or no diabetes. Results may not fully generalize to women, elderly patients >85, or those with severe renal impairment (eGFR <20).
Mechanisms and plausibility: Do results align with the known pharmacology? SGLT2 inhibitors reduce preload and afterload, improve cardiac energetics, and have anti-fibrotic effects — mechanistic plausibility strengthens confidence in the findings.
Limitations to acknowledge:
- Variation in background medical therapy across trials conducted years apart
- Short follow-up relative to chronic disease course
- Underrepresentation of patients with HFmrEF/HFpEF at time of early trials
Example of a clinical bottom line statement
“Moderate-to-high certainty evidence supports the use of SGLT2 inhibitors in HFrEF patients regardless of diabetes status, with a consistent ~25% relative risk reduction in CV death or worsening heart failure.”
9. Update the Review as Needed
Systematic reviews are not static documents. The evidence base evolves continuously.
When to update a systematic review:
- New large RCTs are published (e.g., EMPEROR-Preserved extending SGLT2i evidence to HFpEF)
- New safety signals emerge post-marketing
- Guidelines change (e.g., SGLT2i promoted to first-line therapy by ESC/ACC)
- Methodological standards evolve (e.g., new GRADE domains)
- A pre-specified update interval is reached (typically 2–5 years)
How to update a systematic review efficiently
- Run an updated literature search from the date of the last search
- Apply the same inclusion/exclusion criteria
- Use living systematic review methodology if the topic is rapidly evolving (e.g., re-running searches monthly and updating online continuously). This method was used extensively during COVID-19 trials and increasingly in cardiology for emerging therapies.
Example
A 2020 systematic review of SGLT2 inhibitors in heart failure would need updating to incorporate the EMPEROR-Preserved (2021) and DELIVER (2022) trials showing benefit in HFpEF. This was a major paradigm shift that would change both the pooled estimates and clinical conclusions of the review.
How is a systematic review article structured?
A systematic review article follows the same structure as that of an original research article. It typically includes a title, abstract, introduction, methods, results, discussion, and references.
How to write the title of a systematic review?
The title should accurately reflect the topic under review. Typically, the words “a systematic review” are a part of the title to make the nature of the study clear.
How to write the abstract of a systematic review?
A systematic review usually has a structured Abstract, with a short paragraph devoted to each of the following: background, methods, results, and conclusion.
How to write the introduction of a systematic review?
The Introduction summarizes the topic and explains why the systematic review was conducted. There might have been gaps in the existing knowledge or a disagreement in the literature that necessitated a review. The introduction should also state the purpose and aims of the review.
What should be included in the Methods section of a systematic review?
The Methods section is the most crucial part of a systematic review article. The methodology followed should be explained clearly and logically. The following components should be discussed in detail:
- Inclusion and exclusion criteria
- Identification of studies
- Study selection
- Data extraction
- Quality assessment
- Data analysis
How do I describe the results of a systematic review?
The Results section should also be explained logically. You can begin by describing the search results, and then move on to the study range and characteristics, study quality, and finally discuss the effect of the intervention on the outcome.
How to write the Discussion of a systematic review?
The Discussion should summarize the main findings from the review and then move on to discuss the limitations of the study and the reliability of the results. Finally, the strengths and weaknesses of the review should be discussed, and implications for current practice suggested.
Sample structure of a systematic review
Here’s a sample structure for a systematic review (note that the disease is entirely fictitious):
Title: Risk Factors for Hankypanky Disease: A Systematic Review
- Abstract
- Background
- Objective
- Methods (search strategy, databases, eligibility criteria)
- Results (number of studies included, key findings)
- Conclusion
- Keywords
- Introduction
- Background on Hankypanky Disease (definition, burden, epidemiology)
- Rationale for identifying risk factors
- Gaps in existing literature
- Objective and research question: “What are the risk factors associated with the development of Hankypanky Disease in [population]?”
- Methods (pre-registered on PROSPERO)
- 3.1 Protocol and registration — PROSPERO registration number
- 3.2 Eligibility criteria — Population, Exposure, Comparator, Outcome, Study design (PECOS framework)
- 3.3 Search strategy — Databases searched (PubMed, Embase, Scopus, CINAHL, Web of Science), search terms, date range, language restrictions
- 3.4 Study selection — Screening process (title/abstract → full text), number of reviewers, conflict resolution
- 3.5 Data extraction — Variables extracted (study design, sample size, population, risk factors, effect estimates)
- 3.6 Quality assessment — Tool used (e.g. Newcastle-Ottawa Scale for observational studies)
- 3.7 Synthesis — Narrative synthesis; meta-analysis if studies are sufficiently homogeneous
- Results
- 4.1 Study selection — PRISMA flow diagram (records identified → screened → eligible → included)
- 4.2 Characteristics of included studies — Summary table of all studies (author, year, country, design, sample size, follow-up, risk factors examined)
- 4.3 Quality appraisal results — Risk of bias summary across studies
- 4.4 Risk factors identified organised by category:
- Demographic factors (age, sex, ethnicity)
- Lifestyle factors (diet, physical activity, smoking)
- Clinical/biological factors (comorbidities, biomarkers)
- Environmental/occupational factors
- 4.5 Strength of association — Effect sizes, confidence intervals, consistency across studies
- 4.6 Meta-analysis (if applicable) — Forest plots, heterogeneity (I² statistic), funnel plots for publication bias
- Discussion
- Summary of main findings
- Comparison with existing literature
- Biological plausibility of identified risk factors
- Strengths of the review
- Limitations (heterogeneity, publication bias, confounding in primary studies)
- Implications for clinical practice and public health
- Conclusion
- Key risk factors identified
- Recommendations for future research
- References
- Appendices
- Full search strings for each database
- PRISMA checklist
- Data extraction form
- Quality assessment scores per study
- Supplementary tables
How do I manage references for a systematic review?
The References section of a systematic review article usually contains an extensive number of references. You have to be very careful and ensure that you do not miss out on a single one. You can consider using reference management software to help you tackle the references effectively. Or, if you’re using an AI writing assistant like Paperpal, you can use the free citation generator to get your citations and references formatted automatically across more than 10,000 styles.
Other Frequently Asked Questions
1. What is a living systematic review?
A living systematic review is a relatively new type of systematic review that is continuously updated as new evidence emerges, rather than being a one-time publication. Unlike traditional systematic reviews, which become outdated over time, living systematic reviews use ongoing surveillance of the literature to incorporate new studies in near real-time. They are particularly valuable in fast-moving fields (e.g., during a disease outbreak) where timely, up-to-date evidence is critical for decision-making. The process relies on automated search alerts, standing review teams, and dynamic publishing platforms to keep conclusions current and relevant.
2. What is the difference between a systematic review and meta-analysis?
The main differences between a systematic review and meta-analysis are as follows:
| Feature | Systematic Review | Meta-analysis |
| Definition | A structured review that identifies, evaluates, and synthesizes all relevant studies on a research question | A statistical technique used to combine quantitative results from multiple studies |
| Main Purpose | To summarize and critically appraise existing evidence | To calculate an overall pooled effect or estimate |
| Data Analysis | May include qualitative or narrative synthesis | Uses statistical methods to analyze numerical data |
| Requirement | Can be conducted without statistical pooling | Usually performed as part of a systematic review when studies are sufficiently similar |
| Example | Reviewing evidence on risk factors for hypertension | Combining results of several clinical trials to estimate the effectiveness of a new antihypertensive drug |
3. Which journals publish systematic reviews?
Many journals publish systematic reviews, including broad-scope open access journals like PLOS ONE and BMJ Open and specialist journals like Blood and JAMA Pediatrics. There are a number of journals that focus almost exclusively on systematic reviews, such as:
- Systematic Reviews (BMC)
- Campbell Systematic Reviews
- JBI Evidence Synthesis
4. How do I submit my systematic review to Cochrane Database of Systematic Reviews?
In order to get your systematic review published in Cochrane Database of Systematic Reviews, you must follow these steps:
- Submit a Proposal: First, submit a proposal (formerly ‘title’) via Cochrane Editorial Manager to ensure your topic is relevant and not already being covered. Minimum two authors are required.
- Develop a Protocol: Only if the proposal is accepted, you must write a detailed protocol (plan) for your review.
- Register and Review: Your protocol is published, and you then conduct the review using RevMan software.
- Peer Review: The completed review goes through rigorous peer review, and you may have to revise it multiple times.
Note that Cochrane Database of Systematic Reviews does not accept unsolicited complete manuscripts.
This article was originally published on April 29, 2015, and updated on May 16, 2026.